Multiple myeloma is a relatively uncommon blood cancer primarily affecting the blood, bone marrow, and lymph nodes, and may sometimes create an actual tumor. The American Cancer Society estimates that 30,330 new cases of multiple myeloma will be diagnosed in the United States in 2016, and 12,650 patients will die from the disease. More than 77,000 individuals are living with multiple myeloma in the United States today.
A Type of Blood Cancer
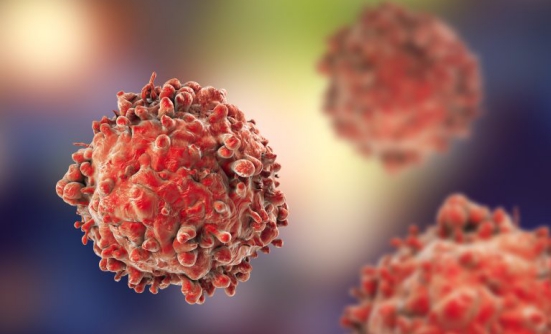
Multiple myeloma develops when abnormal plasma cells (cells that develop from the B lymphocytes in our immune system) transform and grow uncontrollably, preventing healthy cells from growing in the bone marrow. These abnormal cancerous plasma cells, called myeloma cells, make large amounts of the same antibody, which accumulate in the blood and urine and can lead to damage to the kidneys and other organs.
In time, the myeloma cells accumulate in the bone marrow and suppress the growth of healthy white blood cells, red blood cells, and platelets. When the myeloma cells accumulate in solid bone, they cause holes within the bone (called “lytic lesions”), which compromise the strength of the bone.
Risk Factors
The following factors may increase the risk for multiple myeloma:
- Age. Multiple myeloma is more common in older adults
- Gender. Men are slightly more likely to have multiple myeloma than women
- Race. Multiple myeloma is more than twice as common in blacks than in whites
Other factors, including a family history of multiple myeloma, exposure to radiation, obesity, and other plasma-cell diseases, such as monoclonal gammopathy of undetermined significance (MGUS), may increase the risk for multiple myeloma.
Individuals with MGUS have an abnormal plasma protein antibody in the bone marrow (called “monoclonal immunoglobulin M protein”). Although people with MGUS do not have any other signs of multiple myeloma, they have a 1% chance of developing multiple myeloma or lymphoma.
Studies have shown that most patients with multiple myeloma have a genetic mutation (alteration) in their blood cells: either certain parts of chromosome 13 are missing or parts of 1 chromosome have been switched for another.
Symptoms
The most common symptoms of multiple myeloma are bone-related and include pain, bone weakness, and bone fractures. Other symptoms include high calcium levels in the blood (called “hypercalcemia”) that can cause muscle weakness, confusion, dehydration, and kidney problems.
The overaccumulation of abnormal blood cells in the bone marrow that is typical in multiple myeloma crowds out healthy red blood cells, which leads to anemia; white blood cells, which leads to leukopenia and the risk for infection; and platelets, which result in thrombocytopenia and increased risks for bleeding and bruising.
Diagnosis
If the symptoms suggest that a person may have multiple myeloma, the doctor will order diagnostic testing. These typically include blood and urine laboratory testing to measure antibodies, immunoglobulins, and protein light chains (that is, proteins produced by blood cells); x-rays, MRIs, PET scans, CT scans, and bone or skeletal surveys to detect bone destruction; bone marrow biopsy with flow cytometry (to measure the cells in bone marrow, lymph nodes, or blood); and cytogenetics (to measure chromosomes) to see if there are multiple myeloma cells in the body.
Multiple myeloma is diagnosed conclusively if 60% or more abnormal plasma cells are in the bone marrow, or if 10% abnormal blood cells are in the bones in addition to the presence of either anemia, hypercalcemia, poor kidney function, holes or lytic lesions, or an increase in protein light chains.
Treatment of Multiple Myeloma
The treatment options for multiple myeloma include watchful waiting (surveillance), chemotherapy, targeted therapies, chemotherapy combined with targeted therapies, radiation therapy, and stem-cell transplantation. The factors that affect the choice of a specific treatment include the stage of the disease, the patient’s age and overall health, and the symptoms.
Radiation therapy. Radiation therapy can be used to treat localized multiple myeloma or bone pain.
Chemotherapy. Most patients with multiple myeloma receive some form of chemotherapy, which may consist of a single drug or several drugs given in combination. Recently, experts have begun to use drug combinations instead of single drugs for the treatment of multiple myeloma. Common chemotherapy drugs for multiple myeloma include Treanda (bendamustine), BiCNU (carmustine), Cytoxan (cyclophosphamide), Decadron (dexamethasone), Doxil (doxorubicin), Etopophos (etoposide), Alkeran (melphalan), Deltasone (prednisone), and Oncovin (vincristine).
Stem-cell transplantation. Also known as a bone marrow transplant, stem-cell transplantation involves an infusion of healthy stem cells collected from the blood, bone marrow, or umbilical cord blood into the patient’s body. Stem cells used for transplantation can come from the patient’s own (autologous) tissue or from a donor whose tissue closely matches the patient’s (allogeneic). The stem cells allow healthy new blood cells to develop in the bone marrow and fight multiple myeloma cells.
Surgery. Although surgery is rarely used for multiple myeloma, placing metal plates or rods for support or to prevent further bone fractures may be performed.
Supportive therapies. Many supportive therapies can be used to reduce the symptoms and complications associated with multiple myeloma. These include:
- Bisphosphonate drugs to prevent bone lesions, reduce pain, and lower bone fracture risk
- Erythropoietin and darbepoetin to treat anemia
- Immunoglobulin replacement therapy to boost the immune system
- Plasmapheresis to remove myeloma proteins from the blood
Drug Therapy
Multiple myeloma, in general, is not yet curable, but the progress made in targeted therapies and transplantation have made it more treatable than ever, allowing patients to live longer high-quality lives.
Targeted therapies are designed to treat specific genes, proteins, enzymes, or tissue environments of myeloma cells to block the cancer from growing and spreading. Several types of targeted therapies are now available for this disease:
- Immunomodulatory drugs cause an immune response against the cancer, usually with few side effects
- Proteasome inhibitors target enzymes called proteasomes that help to slow or stop the growth and development of multiple myeloma cells
- Histone deacetylase (HDAC) inhibitors are a new type of therapy that fights certain enzymes on the cancer cell and inhibits cancer development
- Monoclonal antibodies are the newest type of immunotherapies for multiple myeloma
Combination therapies of 2 or 3 drugs are now the preferred strategy for patients with multiple myeloma. Experts have recently suggested that using 3-drug combinations that include a proteasome inhibitor, an immunomodulatory drug, and a steroid should be considered for newly diagnosed patients with this disease. Several drug combinations are currently approved by the FDA for multiple myeloma.
Targeted Drugs
Velcade (bortezomib), a proteasome inhibitor, was first approved for multiple myeloma in 2003 for patients whose disease progressed after receiving 2 other medications. In 2014, Velcade was approved for patients who have used it before but their disease returned after 6 months.
Thalomid (thalidomide), an immunomodulatory drug, was approved in 2006 in combination with dexamethasone for first-line therapy of patients with multiple myeloma.
Revlimid (lenalidomide), an immunomodulatory drug, was approved in 2006 for patients with multiple myeloma who received at least 1 previous therapy. In 2015, Revlimid was approved as first-line therapy for patients who were just diagnosed with this disease.
Kyprolis (carfilzomib), a select proteasome inhibitor, was first approved in 2012 for patients who received at least 2 previous therapies. In January 2016, Kyprolis was approved for patients whose disease relapsed (came back) after 1 therapy.
Pomalyst (pomalidomide) is another immunomodulatory drug for multiple myeloma; it was first approved in 2013 for patients whose disease progressed after treatment with other drugs. In 2015, Pomalyst was approved in combination with dexamethasone for patients who received at least 2 previous drugs.
Farydak (panobinostat) was approved in 2015 and is the first HDAC inhibitor for patients with multiple myeloma. Panobinostat is an oral capsule and is taken in combination with Velcade and dexamethasone.
Darzalex (daratumumab) was the first monoclonal antibody for multiple myeloma. Darzalex was approved in November 2015 for patients who received at least 3 previous treatments.
Empliciti (elotuzumab) was the second monoclonal antibody approved in November 2015; it should be used in combination with Revlimid and dexamethasone for patients who have received at least 1 previous therapy.
Ninlaro (ixazomib) was also approved in November 2015 and is the first oral proteasome inhibitor, meaning it is a pill taken orally, and is used in combination with Revlimid and dexamethasone for patients who have received at least 1 previous therapy.