As the Director of the Colorado Cancer Screening Program and adviser to Fight Colorectal Cancer, screening for colorectal cancer (CRC) is at the top of my professional radar. But it’s also personal for me, as I have a family history of CRC. I started undergoing colonoscopies when I was 30 years old, based on my mother’s CRC diagnosis at age 40.
Colorectal Screening Guidelines
The United States Preventive Services Task Force (USPSTF) is an independent panel of experts in primary care and prevention who develop recommendations for clinical preventive services; their guidelines are most frequently used by the medical and insurance communities to determine which tests are most effective for patients. The following is reflective of their recommendations of approved methods for CRC screening.
Screening for People With Average Risk
There is a variety of CRC screening tests available; the right test will depend on your risk. Your healthcare provider may determine “average risk” for CRC if you:
- Are between 45 and 75 years of age
- Have no family history of CRC
- Have no personal history of CRC
- Do not have a hereditary cancer syndrome (such as Lynch syndrome), polyps, or other gastrointestinal disease.
Option 1: Colonoscopy
Colonoscopy is a common procedure for CRC screening. While you are sedated, a flexible fiber-optic tube is inserted through the anus to examine the colon. During the colonoscopy, the doctor can find and remove polyps.
It is important to note that for those with a high risk for CRC, colonoscopy is necessary and the only option for effective screening.
Option 2: Stool-Based Tests
For people with average risk who are hesitant to undergo colonoscopy, at-home stool-based tests can be a great option. At-home tests offer more privacy, flexibility, and affordability. This type of test is intended for adults ages 45 to 75 with average risk for CRC (those without a personal history, a family history, or a hereditary condition).
Yes, these tests are indeed testing your stool, and while it may carry an “ick” factor for some, they’re relatively simple to perform and come with sanitary equipment that makes them quick and easy.
There are 3 general categories of stool-based tests:
- Fecal immunochemical test (FIT or iFOB): Finds traces of blood in the stool using antibodies
- Guaiac fecal occult blood test (gFOBT): Detects hidden blood in the stool using a chemical called guaiac
- FIT-stool DNA (FIT/DNA or sDNA): Screens for DNA alterations associated with CRC on the test (most people may be aware of this test as the Cologuard test).
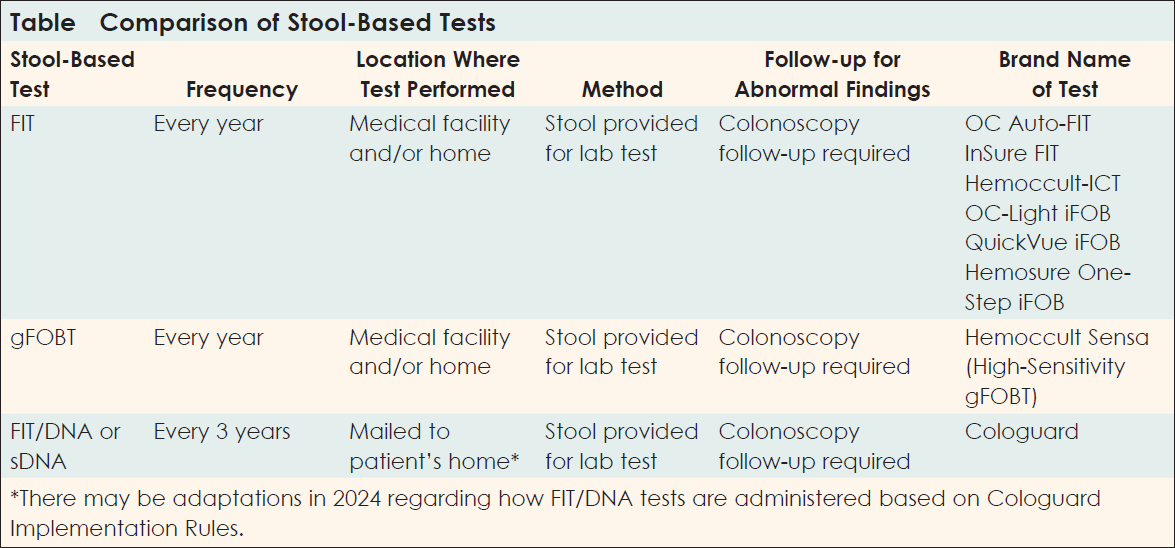
What Are the Differences Between Stool-Based Tests?
Let’s look at some of the details of stool-based tests (Table). Prior to selecting a stool-based test, you will want to consider these factors:
- Frequency (How often does the test need to be performed?)
- Location (Where does the test need to be performed?)
- Methods (Can the test be sent off to a lab, or is a direct visual of the colon needed?)
- Follow-up procedures for abnormal findings (What are potential next steps?).
Sensitivity and Specificity of Stool-Based Tests
Before deciding to use a stool-based test for CRC screening, you should have a discussion with your doctor about each test’s clinical performance. In scientific terms, this is called the sensitivity (the test is truly positive) and the specificity (the test is truly negative). This is important, because if you’re relying on a stool-based test for CRC screening, you want it to be as accurate as possible.
FIT
The FIT is quite sensitive in detecting CRC and can also detect some advanced adenomas (the type of lesion or polyp that is likely to become cancer). It has relatively high specificity, meaning it’s less likely to produce false-positive results compared to some other tests. FIT is considered an effective CRC screening method, particularly for its ability to detect blood in the stool, which may be a sign of CRC or adenomas.
FOBT
FOBT has been on the market longer than FIT and FIT/DNA. While FOBT is now less commonly used, it remains an effective, approved test for CRC screening and has a high specificity for detecting CRC.
FIT/DNA or sDNA Tests
FIT/DNA, or sDNA tests, are highly sensitive and can detect CRC and advanced adenomas. They also look for specific DNA markers associated with CRC. While sDNA tests are sensitive, they may have lower specificity than FIT or FOBT, which can result in more false-positive results.
A Few Facts
- 1 in 23 men and 1 in 25 women will be diagnosed with CRC in their lifetime.
- CRC impacts American Indian, Alaskan Native, Black, and LGBTQ+ communities disproportionately.
- 1 in 3 adults who are eligible for CRC screening is NOT up to date with their screening.
Sources
- American Cancer Society. Colorectal Cancer Facts & Figures 2023-2025. www.cancer.org/research/cancer-facts-statistics/colorectal-cancer-facts-figures.html
- American Cancer Society. Key statistics for colorectal cancer. January 17, 2024. www.cancer.org/cancer/types/colon-rectal-cancer/about/key-statistics.html
The Costs of Stool-Based Tests
The good news is that stool-based tests are typically covered by insurance for most individuals and are all effective in detecting CRC. For uninsured patients, the FIT and FOBT are relatively inexpensive to pay out of pocket for a test.
For people who meet income qualifications and wish to use a FIT/DNA test, the company Exact Sciences sponsors a financial assistance program.
A Note for High-Risk Individuals
I must remind everyone that stool-based tests are recommended by the USPSTF and other professional organizations only for people at average risk between 45 and 75 years old. Colonoscopy is the only screening recommendation for those who have signs or symptoms of CRC; those at increased risk due to a family history of CRC or a hereditary cancer syndrome; or those with a personal history of CRC, polyps, or gastrointestinal disease. This includes young adults who are not yet 45 years old.
Stool-based screening methods do not apply to this young population, nor do they apply to anyone experiencing signs and symptoms of the disease. In this case, colonoscopy is the only option—and it should be done promptly.
A Final Thought
It’s important to know and understand your CRC risk. It’s also important to understand CRC screening options based on your risk.
To close, I’d like to offer a quote from Syd Winawer, MD, DrSc, the long-time chief of the Gastroenterology and Nutrition Service and chairman of the Cancer Control and Prevention Program at Memorial Sloan Kettering Cancer Center. He said: “The best screening test is the one that gets done, and gets done well.”
My advice to everyone about screening for CRC: Don’t delay this important conversation with your healthcare provider, family, and friends; it could save a life.
Symptoms of Colorectal Cancer
If you have any of the following signs or symptoms of CRC speak to your healthcare team about the need for a colonoscopy. It’s important to note that stool-based tests are not recommended for people with signs and symptoms of CRC.
- Blood in your stool
- Change in bathroom habits/more frequent diarrhea, constipation, or feeling like the bowel can’t empty completely
- Unexplained weight loss (typically 10 or more pounds)
- Bloating or gas pain
- Fatigue
- Recurring abdominal cramps or lower back pain.
Source
- American Cancer Society. Signs and symptoms of colon cancer. February 8, 2021. www.cancer.org/cancer/latest-news/signs-and-symptoms-of-colon-cancer.html
About the Author
Andi Dwyer, BS, is the Director and a founding member of the Colorado Colorectal Screening Program (CCSP), where she implemented the country’s largest patient navigation screening program within the safety net clinics in Colorado. Ms Dwyer is also a Chair of the National Navigation Roundtable and a member of the Academy of Oncology Nurse & Patient Navigators Leadership Council.