Some patients who have been diagnosed with chronic lymphocytic leukemia (CLL), a type of blood cancer, have slow-growing or “indolent” disease. These patients can be watched or monitored for months to years before needing treatment. This close monitoring, called “active surveillance,” includes regular medical examinations and blood work to determine whether the disease is stable or has begun to progress.
Experts in the management of CLL have worked together to write the International Workshop on Chronic Lymphocytic Leukemia (iwCLL) guidelines. These guidelines help cancer specialists, known as oncologists, decide whether to start treatment for patients with CLL. According to the iwCLL guidelines, patients who require treatment with medications have ≥1 of the following:
- Symptoms of CLL:
- Extreme fatigue
- Night sweats for ≥1 months with no signs or symptoms of infection
- Unexplained weight loss of ≥10% in the past 6 months
- Low-grade fever
- Lymph nodes that are getting larger based on clinical examinations
- “Extranodal” CLL, which is disease outside of the patient’s lymph nodes (eg, in the skin, kidneys, lungs, or spine)
- Increase in spleen size
- Increase in lymphocyte (white blood cell) count, known as “lymphocytosis”
- Evidence that the bone marrow is failing to produce blood cells based on development or worsening of:
- Anemia: red blood cell count of <10 grams per deciliter (g/dL) and/or
- Thrombocytopenia: platelet count of <100,000 per microliter (μL)
- Unresponsive autoimmune anemia and/or thrombocytopenia.
When developing appropriate treatment plans for patients with CLL, oncologists also use staging systems. Two CLL staging systems—the Rai Staging System and the Binet Staging System—are used worldwide. In 2016, a new predictive model, called the CLL International Prognostic Index (CLL-IPI), was introduced. This tool helps oncologists use a more targeted approach to the management of CLL.
The Rai Staging System classifies CLL into 3 risk groups. In this system, patients with “low risk” CLL have a high lymphocyte count only. Patients with “intermediate risk” CLL have a high lymphocyte count plus either enlarged lymph nodes or an enlarged spleen and/or liver. Patients with “high risk” CLL have a high lymphocyte count plus either anemia (hemoglobin <11 g/dL) or thrombocytopenia (platelet count <100,000/μL).
The Binet Staging System classifies CLL into 3 stages:
- A Stage
- No anemia or thrombocytopenia
- Fewer than 3 areas of lymphoid tissue enlargement
- B Stage
- No anemia or thrombocytopenia
- 3 or more areas of lymphoid tissue enlargement
- C Stage
- Anemia (hemoglobin <10 g/dL)
- Thrombocytopenia (platelets <100,000/μL)
- Any number of areas of lymphoid tissue enlargement.
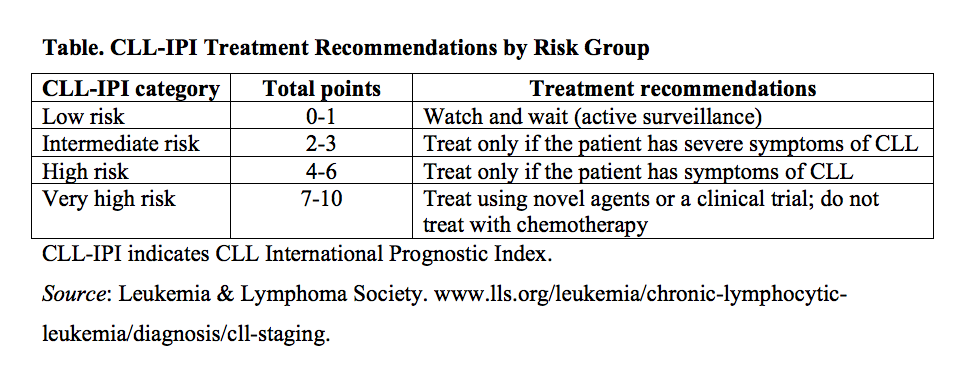
The CLL-IPI model uses results from genetic and biochemical testing, as well as findings from standard examinations and blood tests, to make treatment recommendations for each of 4 risk groups (see Table). Oncologists determine the number of “points” after reviewing all of these test results. It is important for oncologists to routinely reassess the risk levels of patients under active surveillance to determine whether treatment should be initiated.